This information has been put together by the Rotherham Hospital and Community Cardiac Rehabilitation Team as a guide to assist your recovery. It covers a wide variety of information for you and your family.
Experiencing a heart attack can be a frightening event and you may feel worried when leaving hospital, especially if you have left a carefully monitored environment. It is not unusual to find the first few days at home quite daunting and it is important not to expect too much too soon by putting yourself under undue pressure physically and emotionally. It is during this time that we recommend you read the information in this booklet to help you through the first six weeks after your heart attack. This pack is part of your cardiac rehabilitation that is, supporting you to get back to normal.
There is a second booklet that accompanies your recovery and rehabilitation that focuses on ‘Physical activity and exercise after a heart attack’ which should also be referred to.
Cardiac rehabilitation
Before you left hospital you should have been informed that someone will make contact with you when you get home. This will be a practitioner from the Cardiac Rehabilitation Specialist Team whose role is to support you and those close to you over the next few months in understanding the information given to you in hospital, adjusting to life and in making healthy changes. They are also there to assess and monitor symptoms, answer any questions and provide a link between hospital and home.
Cardiac Rehabilitation Practitioners are experienced health and nursing professionals with community and heart qualifications so that each patient can be offered individual information and programmes of cardiac rehabilitation to suit them.
They are in the community and work as part of a team with a Physiotherapist, Dietician and Pharmacist. They are regularly in contact with staff from Rotherham Hospital, the Northern General Hospital and GP practices.
Your cardiac rehabilitation
This pack is part of your cardiac rehabilitation programme to work through at home to help your recovery. You will also be invited to attend an education and/or exercise group. Each patient’s condition is assessed on an individual basis and it may be that you receive visits at home or clinic as well.
This is what we call ‘Cardiac Rehabilitation’. It involves heart health information, emotional support and usually some exercise. Patients who get involved in cardiac rehabilitation tend to have fewer symptoms, less worries and do better overall.
After you have been discharged from hospital you will be contacted by the Cardiac Rehabilitation service to arrange an assessment appointment. You will then receive written confirmation of this and some information about the service and what is available. The cardiologists expect patients to have Cardiac Rehabilitation and this is considered part of your treatment.
When you are seen for your assessment your rehabilitation options will be discussed. These will look at how we can support you in making any lifestyle changes to reduce future risk and includes whether you wish to attend the education and exercise groups and if your medication needs further review at a titration clinic.
The cardiac rehabilitation team often refer patients to other services like: the Get Healthy Rotherham, Sexual Dysfunction Clinic, Mental Health Services and leisure facilities. They also have access to a wide range of information about heart health.
If something is worrying you then it is important, so please ask or write it down to ask when they phone or visit.
The Cardiac Rehabilitation Service is not an emergency service and is only available Monday to Friday, 9am to 5pm. If you are experiencing chest pain that is not relieved by GTN after 10 minutes then you must phone for an ambulance by calling 999.
The heart and your coronary arteries
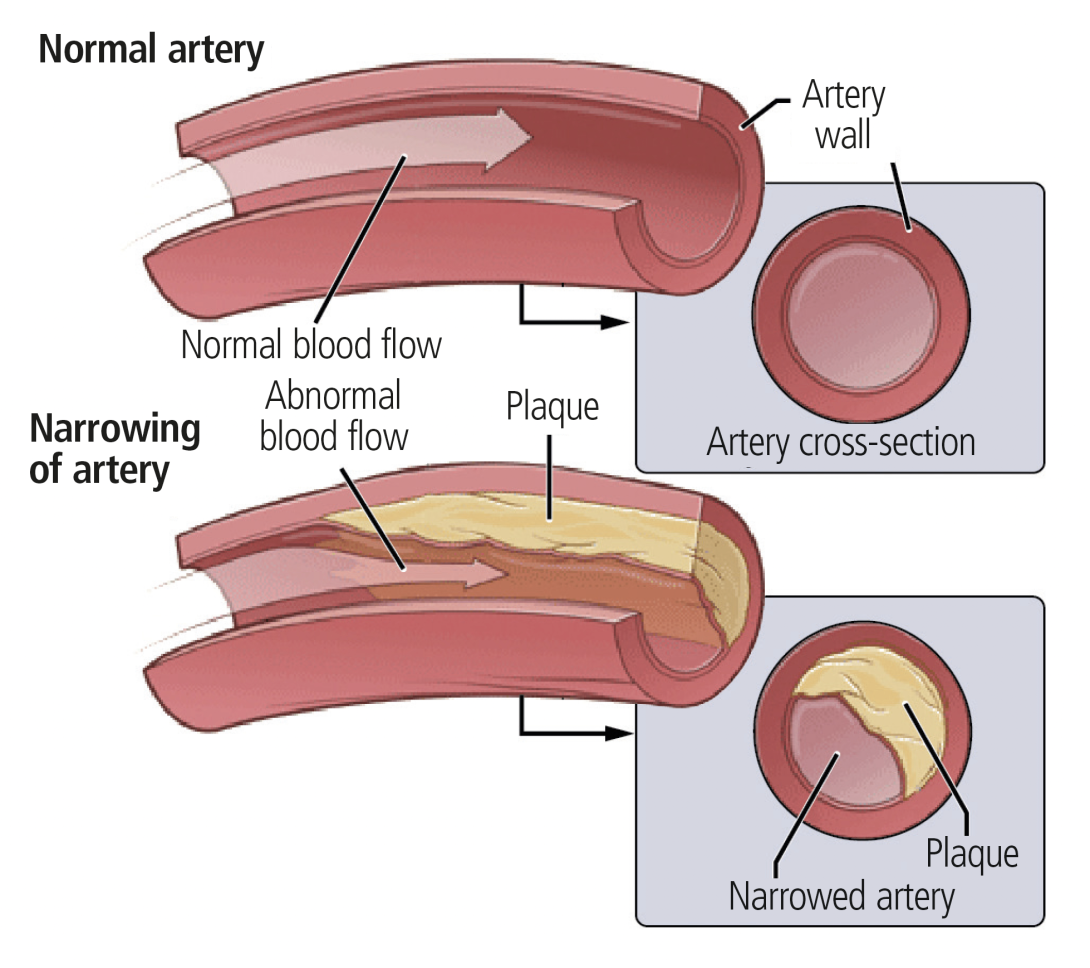
Your heart is a strong, powerful muscular pump. It is made up of four chambers, valves and vessels which drive blood around your body to take oxygen and nutrients to where they are needed. The heart muscle itself also needs a good blood supply for it to perform and to keep it healthy. This is supplied by vessels wrapped around the heart called coronary arteries.
As we get older, the coronary arteries can narrow, a process that starts in our teenage years. The speed at which this happens depends on the number of risk factors we have. The narrowing is due to a build-up of fatty material. This is called a plaque or atheroma. We will discuss your risk factors with you in more detail and these will be covered later on this page.
What is a heart attack?
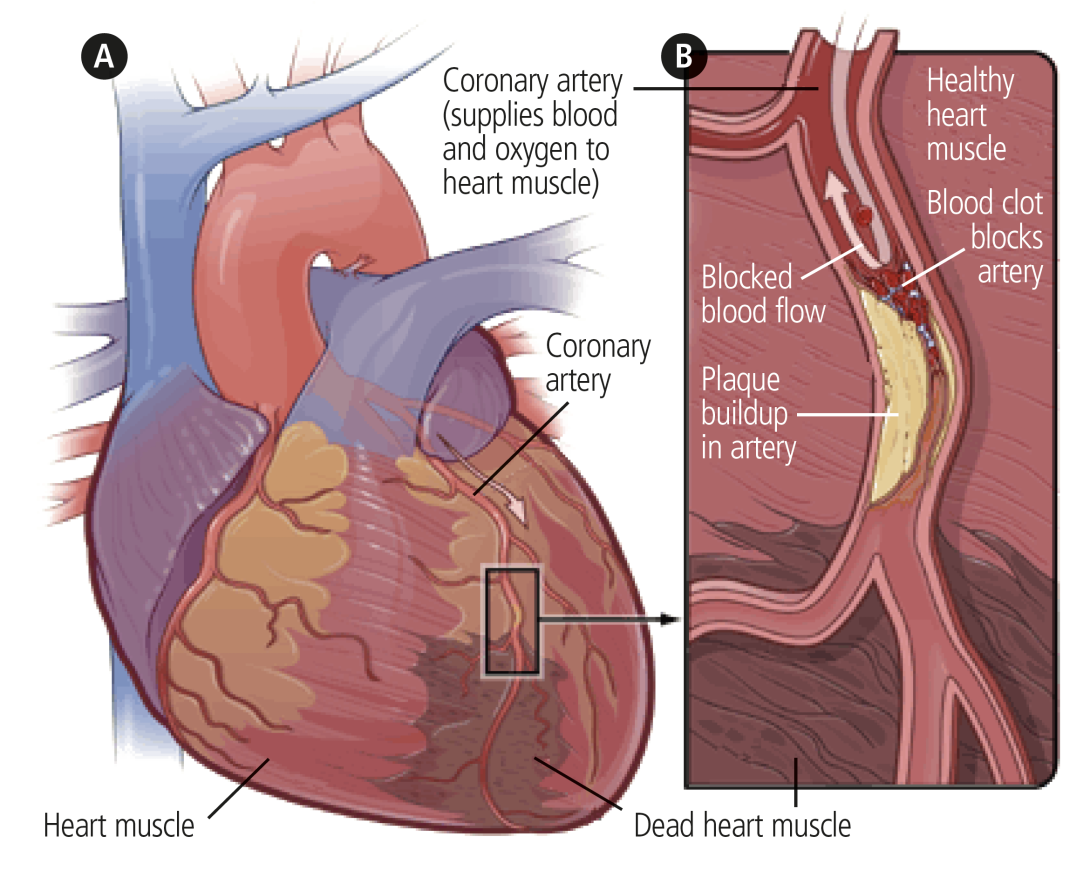
The build up of fatty deposits or plaques inside the wall of the artery can sometimes become unstable. The plaque can then rupture, this triggers the formation of a clot, which is also called a thrombus.
A clot in a coronary artery will block the flow of blood and oxygen to the heart muscle it serves down stream. This leads to the death of heart cells in that area and the symptoms associated with a heart attack. If blood flow is not restored quickly to that area, the part of the heart muscle affected by the blockage will become damaged and eventually develop scar tissue reducing its ability to contract effectively.
Where is the clot now?
Most people will have been given aspirin as soon as a heart attack was suspected. This combined with injections in the stomach when in hospital, the body’s natural clot busters and taking aspirin and/or other anti-platelet medication afterwards, will get rid of the clot over the next few weeks.
People with a certain type of heart attack will be taken directly, by ambulance, to the Heart Centre at the Northern General Hospital, Sheffield. This is so that the blocked artery can be opened with a balloon and stent. After the procedure you will normally be transferred back to Rotherham Hospital.
Not all heart attack patients are suitable for this procedure but this may be considered later once further investigations have been undertaken.
Signs and symptoms of a heart attack
Sometimes there may be no chest pain but other symptoms listed below may be present.
Symptoms of a heart attack can include:
- pain (often severe) in the chest
- heaviness down either or both arms
- discomfort in the centre of the shoulder blades
- pain up into the neck, jaw, teeth
- sudden or gradual onset pain but building
- profuse sweating
- nausea or vomiting
- shortness of breath
- generally feeling unwell
- fainting
- pain not relieved by Glyceryl Trinitrate spray (GTN)
Occasionally a heart attack can be ‘silent’ and produces little or no discomfort. You may not know you have had one until you have a medical test for something else that reveals this information. This often happens in elderly people or people with diabetes.
It is easy to confuse indigestion pain with angina or heart attack pain. Ask yourself if you normally suffer with indigestion, consider what you have eaten and if you have other symptoms that you don’t normally experience
Signs and symptoms of angina
Having a heart attack means that you could possibly experience angina as they are both caused by fatty deposits or coronary heart disease.
A heart attack is normally a complete or near complete blockage by thrombus or plaque in the artery, where as angina is a symptom associated with the narrowing of an artery.
Narrow arteries reduce the amount of blood flow to the heart muscle. This blood supply may be enough when resting, but when you are active both the heart and body muscles need more blood and oxygen. Your heart has to work harder to meet this demand. Because of the narrowing not enough blood can get through and this causes the pain or discomfort known as angina.
Once resting or by taking the GTN spray, the demand on the heart is reduced and the symptoms pass.
Angina is not a mini heart attack and does not leave any lasting damage. However, if symptoms become more frequent or happen unpredictably or at rest then you need to be reviewed by your GP or Cardiac Specialist Nurse.
Symptoms of angina include:
- often bought on by activity, large meals or occasionally emotional stress
- can occur at night or rest often as a result of spasms of the heart blood vessel (different to exertional angina)
- worse in very cold weather/wind
- pain that gradually builds or increases
- often described as discomfort /heaviness / tightness / pressure
- pain in chest, shoulders, back, neck, jaw, arms
- indigestion like symptoms
- shortness of breath
- most symptoms last 1-5 minutes usually not lasting more than 20mins
- eased by rest or GTN
- worsened by anxiety
Managing chest pain
If you experience any of the symptoms described stop what you are doing. If with rest the discomfort does not pass, follow the procedure on how to use your Glyceryl Trinitrate spray (GTN).
Guide on how to manage chest pain
If you are to experience any chest pain please follow this guidance:
- stop what you are doing and rest
- 1 to 2 GTN spray or 1 tablet under the tongue
- if pain is relieved in 5 minutes - 1 to 2 GTN spray or 1 tablet under the tongue
- If pain is not relieved in 5 minutes - call 999 for an ambulance
Dial 999 for an ambulance immediately if you have severe chest pain which is unbearable or similar symptoms to when you had your heart attack.
General guidance when using Glyceryl Trinitrate Spray (GTN)
This is usually prescribed, although tablets that are placed under the tongue are also available. Their action is the same but spray is more convenient.
- Take note of the expiry date. GTN spray should not be used after this date. GTN tablets should be replaced 8 eight weeks after opening the bottle. You are advised to mark this date on the bottle although blister packs are more commonly used now.
- Make sure you always have your GTN with you in case it is needed. If using tablets keep them in their original bottle and do not mix them with others. Do not store in a warm place.
- Angina pain occurs when not enough oxygen is available for the heart. It is often, although not always, related to exertion or change in temperature. GTN works by improving blood flow to the heart, increasing its oxygen supply. GTN is not habit forming. Spray one dose or place one tablet under the tongue.
- You may experience a headache or dizziness. Sitting down whilst using GTN may lessen these effects. If a tablet is used you may discard the undissolved portion of the tablet, spit out or swallow, as soon as the chest pain has eased to reduce side effects.
If you find that a particular activity always causes chest pain, use of the GTN before the activity may prevent the pain occurring.
After a heart attack
Once a heart attack has been diagnosed you may undergo a number of investigations such as an Echocardiogram, Myocardial Perfusion Scan or Exercise Tolerance Test and an Angiogram. These tests look at the blood supply to the heart and also the heart’s pumping ability. This helps the doctors assess the extent of any possible disease or damage.
Your heart is a very strong muscle and your body will replace the area of the heart muscle that is damaged with scar tissue. This takes from a few days to a few months, after this time many patients’ hearts are found to be working just as well as before. This recovery period gives you the opportunity to review your lifestyle and start to make changes in your life that will reduce the risk of further heart problems.
In many cases these changes can lead to a healthier and more fulfilled life. The Community Cardiac Rehabilitation Team can help you through this period with advice, education, exercise and support however your help and commitment are also needed to reduce the risk of this happening again
Myths
My heart doesn’t work as well now
False. Having a heart attack means you may have some scar tissue develop in the muscle down stream from the blocked artery. This is a small area and not the whole of the heart. The scar tissue is strong and very unlikely to cause problems. The rest of the heart muscle compensates for the damaged area.
I must try to keep my heart rate as low as possible
False. Keeping your heart rate low would mean avoiding certain activities, excitement, and exercise. This is not good for your recovery or your heart. The faster your heart rate is, does not mean it wears out more quickly.
Stress and excitement are not good for my heart
False. Avoiding all excitement would be very miserable and avoiding things that would be fun because of fear of stress can lead to feeling down.
Angina is like a mini-heart attack
False. Angina is not a mini-heart attack and it does not leave any lasting damage.
I must be careful what I do
False - in time. It is important to be careful during the first few weeks after your heart attack to not rush straight back into everything you were doing before it happened. There is no reason why in time you shouldn’t get back to your normal daily activities, for most people this is normally by six weeks. Build up every activity you do from scratch increasing a little more each day.
Stress causes heart attacks
False. It is unhelpful to blame stress for your heart attack. Stress does not increase the speed at which we get fatty deposits (the cause of heart attacks) in the arteries. Stress over a long period of time may mean we chose unhealthy activities over the healthy ones. It is these activities that increase the speed of fatty deposits building up, for example we may eat more of the wrong foods, drink more, smoke more and take less exercise.
Once I have had a heart attack there is nothing I can do
False. There are many things you can do to reduce the risk of you having further heart problems. By making a few healthy lifestyle changes and taking the medication and attending all your appointments, many people have a healthier and more fulfilled life after their heart attack than they did before. It is not the beginning of the end.
I must take it easy and rest now
False. It is important to live as actively as you can, to reduce further problems in the future.
Exercise puts the heart under unnecessary strain
False. Exercise of the right intensity improves the ability of the heart to function and make day to day tasks easier to complete. The more you exercise the stronger your heart becomes.
It is only a matter of time before I have another heart attack
False. Having one heart attack does not mean you will have another. This is especially so if you take your medication and make healthy lifestyle changes.
Week 1 - Dos and Don'ts
During the first few days at home, your activities should be similar to those which you were doing during your last few days in hospital. You should remain within the home environment and don’t go outdoors if the weather is very hot or very cold.
Every activity that you do has an energy requirement and some things use up more energy than others.
Many people will want to go back to caring for their family and take up household duties immediately. This can lead to doing too much too soon, leaving you feeling tired.
Do not feel guilty about leaving housework, let other members of the family take their share of household duties for the first few weeks.
Give yourself time to recover and do not do too much at a time. It is good to be active and if you feel well you may feel like doing a lot more but it is important to build up gradually as your heart is still repairing itself. For example do not do all activities suggested in one day.
Try to avoid one task straight after another and pace yourself. The following will help to achieve a balance.
Things you should do
- Get up and get dressed every day.
- Usual personal hygiene care. A shower would be more preferable to a bath. Use a stool or chair in the shower if necessary. Use lukewarm water.You can shampoo your hair.
- Walk around the house and garden.
- Walk up and down stairs at a comfortable pace.
- Watch TV, radio, play cards or read.
- Receive visitors at home, but not more than two visitors a day.
There is additional information on activity and exercise following your heart attack.
- Aim to get six to ten hours sleep and take a rest every day. Your body does most of the repair work while you are sleeping. At the moment it has more repairs to do than usual, so you need your rest. Don’t worry if you are easily tired at this stage. It’s your body’s way of persuading you to rest. It will pass in time. If you are unable to sleep when taking a rest don’t worry, just relax, read or listen to music.
- Deskwork for short periods.
- Cooking light meals.
- Light housework (washing a few pots, light dusting)
Things you shouldn’t do
- Don’t overdo things which make you so breathless you can’t have a conversation.
- Don’t ignore chest pain. If you have pain in the chest which doesn’t go away in 10 minutes despite using GTN and doing all the things recommended, follow the advice given and dial 999.
- Initially avoid going outside on cold, windy days. Your heart has to work harder and some people find that breathing in cold air can bring on angina pain. If you have to go out you can use a scarf over your mouth to provide some protection.
- Drive for 1 or 4 weeks after your heart attack depending on if you have had a stent or not.
- No vacuuming, bed making, carrying heavy loads of washing or hanging out washing.
- Lift or push heavy items. Don’t lift heavy objects that make you strain or grunt, such as heavy pots, full rubbish bags, furniture or heavy shopping, for the first few weeks. If you have to hold your breath to lift something, it’s too heavy.
Getting back to normal
Driving
The DVLA states:
- If you have had a stent (that was successful) whilst in hospital for your heart attack and have no problems afterwards, then you can drive one week from the date of your stent.
- If you have had a heart attack but the stent was not successful, you are unable to drive for 4 weeks.
- If you have a heart attack but no stent (PCI), you are advised not to drive for 4 weeks from the date of your heart attack.
- If you have had a stent (PCI) without a heart attack, you are able to drive after one week if it was successful and you do not need further treatment.
None of these treatments/events require you to let the DVLA know but you do need to let your insurance company know.
If your ejection fraction after a heart attack is 40% or less then guidance is to not drive for 4 weeks.
For holders of group II-HGV/PSV licence
You must notify DVLA for the heart attack and or stent, you are disqualified until you meet the criteria at 6 weeks where you can be relicenced if you have had a satisfactory Echocardiogram result, met requirements on an exercise test and do not hold any other disqualifying conditions.
For more information contact the DVLA via telephone on 0300 7906802 or see the DVLA website.
Work
Some people are ready and able to return to work around six weeks after their heart attack. This depends on the type of job you do, the severity of your heart attack, recovery and if you are still having investigations.
If you have a physically demanding job it may be nearer 3 months before you are advised to return.
Many employers will consider reducing hours for the first few weeks then gradually increasing back to your normal amount.
Sex
Sex is no different to any other type of exercise and if you can walk about 300 metres on the level and comfortably climb two flights of stairs without getting chest pain or becoming breathless, it is normally safe to start having sex.
For most people this is from two to three weeks after your heart attack or when you feel ready.
Sexual intercourse creates the same demand on the heart as light house work and the chance of having a heart attack during sex is extremely rare.
If you have angina on physical exertion, here is some helpful advice about sexual activity:
- Avoid having sex within two hours of a heavy meal or alcohol.
- Keep the bedroom warm and avoid cold sheets.
- Choose a relaxing atmosphere and avoid sex if feeling tense or tired.
- Use a comfortable position and consider getting your partner to take a more active role.
- Have your GTN spray with you in case it is needed.
- If you suffer with angina during intercourse, follow GTN advice.
- Taking your GTN spray prior to intercourse in the future may prevent chest discomfort. If this is happening on a regular basis please see your GP.
- If you have taken Viagra or an equivalent drug, do not use your GTN spray.
Coronary heart disease and some of the medications used to treat it are known to cause erectile dysfunction (impotence) in some men.
This can be as high as three in five. Although anxiety about having another heart attack during sex can affect it, it certainly isn’t ‘all in the mind’.
If you find your sex life is affected, talk to your doctor or nurse, they want to help and understand it is important to you.
There are a variety of treatment options available. It is important to seek medical advice as drugs such as Viagra cannot be taken by patients on certain heart tablets, especially nitrates. Please discuss this with your Cardiac Nurse or GP.
Travel and holidays
If you are travelling by car, try to break the journey every few hours.
UK holidays are fine but please discuss with your Cardiac Nurse or GP for advise prior to travelling. European holiday’s aren’t normally advised until 10-12 weeks after your heart attack, but this can vary from each airline and insurance company, especially if you are still having investigations.
Long haul flights may not be advised until six months in some cases. Carry a copy of your current medication and ECG if you have one.
Make sure you carry your medication in your hand luggage ensuring you have enough for the trip. Depending on terrorism risk, this advice can vary, please check with the airline you are travelling with. Some airlines may require a letter from your GP confirming you need to carry medication in your hand luggage. Allow plenty of time and try not to carry heavy bags.
When taking out holiday insurance you need to inform them you have had a heart attack.
112 is the single emergency telephone number for the European Union. In countries where 112 is not the standard emergency telephone number, callers will generally have their calls redirected to the local emergency telephone number if it exists. For this reason it is important to familiarise yourself with the local number when you arrive at your destination.
Most mobile phones can dial 112 calls when the keypad is locked, without a SIM card or instead of the PIN. When 112 is used dialled from a mobile phone in the UK, it is possible to locate the phone to within 5 meters if you do not know where you are.
The British Heart Foundation have a list of sympathetic insurers for those who have heart conditions if you have difficulty getting insurance.
The new EHIC (European Health Insurance) card replaces the E111 (no longer valid) for travel within a European Economic Area (EEA).
It can be used for the cover of any necessary medical treatment due to accident or illness within an EEA. It will not always cover all medical costs and is in no way a replacement for holiday insurance.
In case of emergency (ICE)
The emergency services now recommend that everyone has an ‘ICE’ number in their mobile phone.
This is the telephone number of a person you want contacting in case of emergency. This may be your next of kin, spouse, partner, children or friends.
You need to enter into your mobile phone the letters ICE in front of the name of the person you wish to be contacted. For example this would look like ; ‘ICE Sandra’. It is possible to have ICE 1 Name, ICE 2 Name and so on.
The emergency services can then scroll down your address book and phone through your list of ICE numbers until they got hold of someone to alert them of your situation and to obtain any necessary medical information.
Feelings after a heart attack
Stress
It is normal to worry after a heart attack or any other frightening experience! Obtaining more information about worry and stress can help many people to handle it better.
Stress is difficult to define and varies from person to person. Stress can come on very quickly or be ongoing. Stress is when something unpleasant happens around us that puts us in a state of strain. Stress is beyond an individual’s ability to cope; this may be in general or in specific situations. If you find you are having difficulty coping, this is when you need to look at ways to overcome your stress.
Physical signs of stress include:
- headaches
- bowel or bladder problems
- muscle tension or pain
- breathlessness or palpitations
- stomach problems
- dry mouth
- sweating
- light-headed or feeling dizzy
- tingling in body
- sexual problems
Emotional signs of stress include:
- feeling irritable
- feeling anxious or tense
- feeling in a low mood
- lack of concern or interest
- feeling low in self-esteem
Effects on what you do include:
- temper outbursts
- drinking or smoking too much
- changes in eating habits
- withdrawing from usual activities
- becoming unreasonable
- becoming forgetful or clumsy
- rushing around
- difficulty concentrating
Long-term stress is known to be bad for our health. It may also be the cause of illnesses such as irritable bowel syndrome, psoriasis, migraine, tension, headaches and it can also make other conditions worse.
Ways to help yourself
- Practise simple relaxation techniques you may want to set aside a few minutes each day to sit quietly and take deep breaths to allow your body to relax.
- Take regular exercise building up to 30 minutes - see Physical Activity and Exercise After a Heart Attack booklet.
- Eat a well balanced diet try to eat at least five portions of fruit and vegetables a day and reduce the amount of sugar and processed food and take time over your meals.
- Find a hobby or an interest that you enjoy and set time aside each week.
- Take a holiday; it is good to have something to look forward to.
- Don’t use alcohol to help cope with your stress.
- Read relevant books on self help techniques.
- See a doctor or other health professional if the problem continues. If you have tried to help yourself and stress is still causing you a problem, or it is getting worse, then contact your GP.
Relaxation
Relaxation has been proved to help recovery after a heart attack and will also ease any stress, anxiety or depression you may be feeling.
The health benefits of regularly practising relaxation are; lowered blood pressure, slower heart rate, increased feelings of being in control, lower bad cholesterol level, reduced angina symptoms, better sleep and reduced pain.
A lot of people say they relax by reading, watching TV or listening to music. Whilst these activities are good to include as part of your daily routine this kind of relaxation isn’t deep enough to bring about the health benefits discussed.
It takes practice to learn how to relax but it is recommended that you try this up to twice a day. Like anything, relaxation takes time, it may feel that very little is happening but keep going! It can take up to 12-16 weeks to get the full benefits.
Depression
Stress is a well known trigger for depression and so it is quite common to feel low in mood after a heart attack. This can become worse for a while after you get home, mainly because it takes time for what has happened to sink in.
Facts about depression
Depression is one of the most common mental health problems and also one of the most easily treatable mental health conditions. It occurs more frequently in women – one in four, as opposed to one in ten of men.
Signs of depression include:
- fatigue or loss of energy
- feelings of helplessness
- sleeping problems
- difficulty concentrating
- abnormal sadness and weepiness
- irritability
- poor motivation
- poor appetite
- feelings of guilt and unworthiness
- loss of enjoyment and interest in activities you would normally enjoy
- some physical aches and pains can occur such as chest pains, headaches and palpitations
- recurrent thoughts of suicide or death
If you are experiencing four or more these symptoms for most of the time over a period of two weeks or more, it is advised that you should seek help.
Self help
The below may help to manage some symptoms:
- finding and reading information about depression
- using self help materials - either on your own or with the help of the Cardiac Rehabilitation Nurse
- learning problem solving techniques either on your own or with the help of the Cardiac Rehabilitation Nurse
- learning relaxation skills to reduce stress
- learning how to control your breathing
- increasing the amount of physical exercise
- pursuing interests and hobbies
Cognitive behaviour therapy
You will need to talk to the Cardiac Rehabilitation Nurse about this treatment, which helps you to understand and change any current thought patterns which may be contributing to your depression. It is usually done in sessions over a period of weeks.
Medication
Medication is not usually prescribed at first although certain medications can be prescribed to help. These medications are known as anti-depressants, they:
- treat depression by increasing the levels of certain chemicals in the brain
- can reduce the symptoms of depression, but cannot change an individual’s personal situation
- can take two to four weeks to work properly
- they are not usually addictive but may have some withdrawal symptoms if stopped suddenly
- the most effective treatment for depression tends to be a mixture of more than one of these therapies and require the patient to take an active role in their treatment
After a heart attack - investigations
Once a heart attack has been diagnosed you will undergo a number of investigations such as an Echocardiogram, Myocardial Perfusion Scan or Exercise Tolerance Test and in some cases an Angiogram. These tests establish how well your heart is working and assess the extent of any possible damage.
Electrocardiograph ECG
This measures and records the rhythm and electrical activity of the heart. It detects any abnormalities such as previous heart attacks and if the heart is under any strain or is enlarged. Wires and electrodes are connected to the chest, arms and legs these are attached to the ECG machine, a recording is then taken of the hearts signals. This procedure takes approximately five minutes. You may be given a copy to take away with you so that if you have another heart attack the ECG can be compared to see if there are any changes.
Echocardiogram
The term ‘Echo’ may be used for this procedure and it is an ultrasound scan. This can take up to an hour. A probe is moved over the chest which picks up waves of echo off the heart wall and valves. The hearts function can be seen on the screen and it shows how well the heart pumps and if there is any muscle or valve damage.
Exercise tolerance test (ETT)
This is also known as the stress or treadmill test. The test is carried out by walking on a treadmill while having an ECG and your breathing and blood pressure are being recorded. It shows how the heart works during exercise and if the supply of blood meets the heart muscle demand. Every three minutes the speed and slope increases, it takes up to 15 minutes. Be reassured you are able to stop at any point! The procedure normally takes place at four to six weeks after your heart attack, but this test is now used less frequently.
Coronary Angiogram
This is also known as a Catheter Study and may have been done when you had your heart attack. If you need this as an outpatient, it requires a pre assessment appointment usually the week before you have the procedure. On the day of the test you will be admitted as a day case onto the Cardiac Suite. An angiogram can take up to an hour but you need to be on bed rest for a short period afterwards. A local anaesthetic is given in the groin or arm artery and a catheter is fed to the correct position in the heart, dye is then injected and X-rays are taken. It shows any disease, narrowing, blockages (impaired blood flow) in the arteries. Patients normally go home after four hours and the results are usually discussed with you on the day.
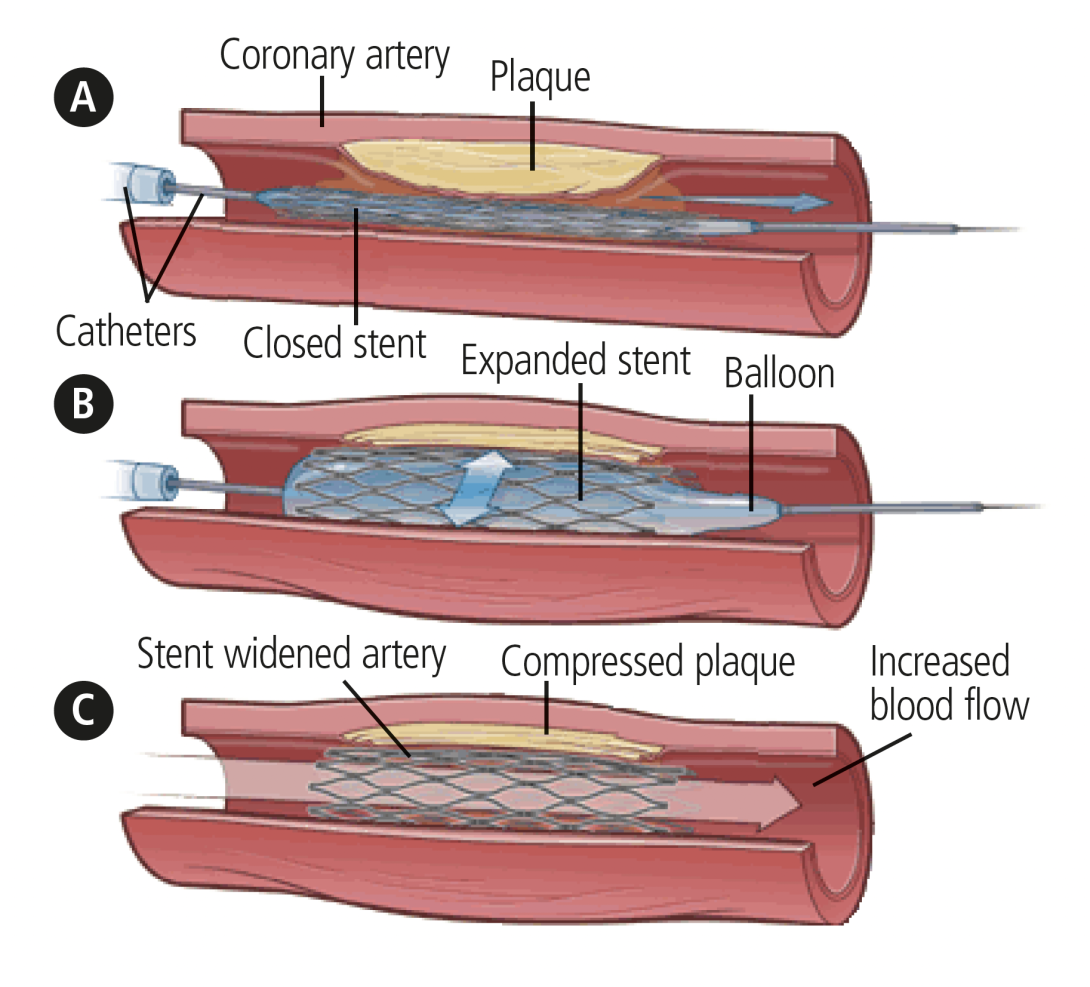
Angioplasty and stents (PCI)
The angiogram procedure is repeated for an angioplasty or stenting with a slightly larger catheter. It takes up to two hours, you may need an overnight stay. (Most preplanned stents are now done as a day case). A balloon is inflated at the artery narrowing and removed or replaced with a wire stent to hold the artery open. Stents are mesh tubes used to prop open narrowed or blocked arteries to improve blood flow to the heart muscle. One or several may be used. They take four to six weeks to fully embed into the artery wall and do not need replacing.
Myocardial Perfusion Scan
This procedure shows how much blood reaches the heart muscle and detects the degree of coronary heart disease or muscle damage. It allows a comparison between resting and exercise conditions. First, the heart is put under stress by exercise or drugs. A radioactive injection is given and X-rays taken shortly after. This process is repeated in an ‘at rest’ condition later or on another day.
After a heart attack - medication for the heart
There are four specific drugs that most people who have had a heart attack will be given. These are anti-platelets, betablockers, statins and ACE inhibitors. This well researched combination reduces the risk of further events and helps reduces symptoms, long term stress and damage on the heart and improve its overall function.
Anti-platelet drugs (Aspirin, Clopidogrel, Ticagrelor and Prasugrel)
Anti-platelets drugs are very important drugs for people with heart disease. These drugs stop the platelets which help in clot formation from becoming sticky and clumping together. Aspirin is often combined with a second antiplatelet drug after stent insertion and heart attacks. These drugs can cause bleeding and bruising and caution is taken with patients who have history of stomach ulcers. Currently it is recomended that anti-platelet drugs other than Aspirin are taken for 1 year following stent insertion.This provides further protection preventing blood clots forming on the stent. Sometimes this can be up to 3 years but on a reduced dose after the stent insertion
Betablockers (Metoprolol, Bisoprolol, Carvedilol)
Beta blockers reduce the heart’s workload by slowing down the heart rate and strengthening contraction. They are used for symptoms of angina, high blood pressure and after a heart attack. They can sometimes cause tiredness, cold fingers and toes, nightmares, dizziness and wheeziness. Men can also experience difficulty with erections (impotence) as a side effect (this can be rectified, please discuss with your nurse).
Cholesterol Lowering Drugs - Statins (Simvastatin, Atorvastatin)
The aim of these drugs are to reduce the level of cholesterol in the blood which reduces the risk of further heart attacks. Side effects can include tiredness, nausea, vomiting, diarrhoea and headache. These drugs work better taken at night as this is when most of our cholestrol is produced.
ACE Inhibitors (Ramipril, Enalapril, Perindopril)
These drugs reduce the workload of the heart and have shown in research studies to lengthen life, reduce hospital admissions and improve symptoms and exercise tolerance. The side effects of these drugs, is that they can lower blood pressure, therefore occasionally cause dizziness also some people experience a dry irritating cough and so may be given an Angio II receptor antagonist (i.e. candasartan, valsartan) instead. It is normal that the dose of ACE inhibitors will be increased over time. this does not mean your condition has worsened. If you were put on the higher dose to start with you are more likely to suffer side effects. You may need blood tests before the dose is increased to check it is not adversely affecting your kidneys.
Other cardiac drugs
Nitrates (ISMO, Imdur, Isotard, Monomil)
These are used to help control angina or breathlessness by relaxing the vessels that feed blood to the heart. They can be in a short acting spray form GTN, or longer acting tablets, isosorbide mononitrate.
Diuretics (Furosemide and Bumetanide)
These help your body to get rid of excess water which if left can cause swollen ankles or breathlessness. You should notice that you pass more urine after taking these tablets. They are sometimes used to treat high blood pressure.
Risk Factors - preventative lifestyle tips that could save your life
Making Positive Changes
The Cardiac Rehabilitation Practitioner will discuss what it may be in your lifestyle or health history that has contributed to you developing coronary heart disease. These are known as risk factors, as many risk factors can be reduced through lifestyle changes. You can hugely reduce the risk of further heart problems by making healthier lifestyle changes, taking the prescribed tablets and by having further treatments.
People who have heart disease and make changes to their lifestyle often enjoy a much healthier and more fulfilled life than before diagnosis.
The causes of heart disease are similar to many other causes of ill health. Making changes in your lifestyle not only reduces your risk of further heart problems but improves your overall well-being.
People who develop heart disease are usually exposed to a number of risk factors which affect the heart and its function. Some risk factors cannot be changed and are out of our control, these are: age, family history, male gender and being of Southern Asian origin.
The risk factors we can reduce and change are:
- smoking
- high cholesterol
- high blood pressure
- diabetes
- obesity
- low activity levels
You are more likely to maintain any changes by choosing one thing at a time to focus on rather than changing everything at once. The risk factors are listed in order of importance, so try tackling them in order on this page.
Smoking
Stopping smoking is the single most positive change you can make to benefit your heart. From as little as 20 minutes after stopping, your risk begins to fall. One of the effects of smoking is that it damages the lining of the artery walls which makes it easier for cholesterol to be taken up, this causes the arteries to narrow.
Some tips to help you keep quit:
- make a date to stop and stick to it
- keep busy (write a list of things to do to fill your time)
- drink plenty of fluids
- increase activity level
- think positively
- change your routine
- make no excuses to stop
- treat yourself if you don’t have a cigarette
- be careful what you eat
- take each day at a time
- seek support from family and friends
- it’s never too late to stop!
Get Healthy Rotherham can offer you support and patients can refer themselves online.
01709 718720
There are a variety of nicotine replacement therapies or medications available to help ease the withdrawal, boost confidence and morale and lessen the urge to smoke. Alternatively you can go to your GP, practice nurse or pharmacy.
High cholesterol
High cholesterol levels increase the speed at which the arteries narrow. This is influenced by the amount of saturated fats in the diet.
Animal fats, lard and dairy products such as butter, hard cheeses and creams are saturated fats.
Cholesterol levels can be lowered by reducing overall fat intake, choosing lower fat options and changing the type of fats you use.
Polyunsaturated fats such as sunflower or corn oil or monounsaturated fats such as olive and rapeseed oil are better for you.
When cooking grill or bake rather than frying. Limit the amount of takeaway food you eat.
Choose oat based or whole grain cereals and increase fruit and vegetables to five a day as these help absorb and remove cholesterol from the body.
Drugs called ‘Statins’ also help reduce cholesterol levels.
Alcohol
Men and women are advised not to drink more than 14 units a week. This equates to 14 single measures of spirits (ABV 37.5%) or, 7 pints of average-strength (4%) lager, or 7 x 175ml glasses of average-strength (12%) wine; with 2-3 units a day for a woman and 3-4 units a day for a man with a few days off a week.
Keeping to recommended guidelines and having a few alcohol free days a week, also means a lower risk of other illness such as liver disease and cancer.
Drinking above the recommended guidelines can increase one of the fats measured as part of your cholesterol.
High blood pressure
Unless your doctor tells you otherwise, your blood pressure should be below 140/90mmHg. However if you have coronary heart disease or a had a heart attack, then it is usually recommended that your blood pressure should be below 130/80mmHg.
Drugs play a large part in controlling blood pressure but diet and exercise make a big impact too. Once controlled, see your doctor or nurse specialist about starting exercise.
Changes in diet such as reducing salt consumption, caffeine and alcohol intake will improve your blood pressure, as well as stopping smoking and losing weight.
Reducing blood pressure lowers the stress and demand on the heart.
Diabetes
Diabetes can be controlled by diet, tablets or insulin. Well controlled diabetes is less likely to cause long term heart problems.
Type II diabetes is often associated with higher cholesterol levels, high blood pressure and obesity.
A small reduction in these reduces blood glucose levels and the risk of diabetic problems. You should be seen regularly by your practice nurse.
Obesity
Obesity is best managed by diet, exercise and, in some situations, medication. Just a 10% reduction in weight can bring huge health benefits.
A healthy diet of balanced foods and controlled portion size is the key. Try to increase fruit and vegetables to five a day and cut down on fats.
It is better to grill and cook at home instead of using ready meals or takeaways as these contain a lot of hidden fat and calories. Alcohol is high in calories and should also be reduced.
Choose whole grain or brown over white carbohydrate options as these take longer to digest, making you feel fuller for longer.
Low activity levels
Low activity levels have a bad effect on all other risk factors. Light activity around the house or garden at frequent intervals during the day is a good starting point.
Walking is a very effective way to keep fit. Once you are well enough you should try to build up to 30 minutes most days of the week, these can be broken in to shorter more frequent sessions.
It is important to build up gradually and listen to your body. If you are still waiting for test results or procedures it is important you follow the guidance of your doctor.
The Physical Activity and Exercise After a Heart Attack booklet provides a good guide on how to build up exercise and activity levels.
The future - what happens next
In the six weeks since your heart attack you may have had some of the investigations discussed earlier and been seen by the cardiac rehabilitation service for an assessment and agreed your cardiac rehabilitation plan.
Most people have also had their hospital outpatient appointment by three months and have completed their cardiac rehabilitation programme.
Following this, your GP and Practice Nurse will offer you ongoing support and also monitor your heart health. It is important to continue to maintain the positive changes you have made and that your appointments are kept.
This is a time where you can consider joining local exercise programmes, walking groups and heart patient support groups.
After discharge additional services and support remain available to you, Stop smoking and local weight support groups can still be accessed.
There is also the Rotherham Heart Support group who meet monthly. This is open to anyone open to anyone with a heart condition, their family and friends.
The aim of the group is to provide a forum for patients to meet together, support each other and share experiences in a relaxed informal setting.
The group is for patients and run by patients. There are regular social events, activities and speakers. The Cardiac Rehabilitation Specialist Nurses will give you more details.
Contact us
Cardiac Rehabilitation Office
Telephone: 01709 427231 or 01709 423257
Coronary Care Unit (CCU)
Telephone: 01709 424760 or 01709 424226
Produced by The Cardiology Department. August 2011.
Revised February 2013, April 2015, Oct 2017, Oct 2018. May 2020, Jan 2022. Revision due Jan 2024. Version: 7.0
©The Rotherham NHS Foundation Trust 2022. All rights reserved